Building Shared Mental Health Literacy in Schools
Building Shared Mental Health Literacy in Schools
Jacqueline Klemke & Nick Praulins, co-founders, Let’s Be Real
In Part 1, we met four voices from the same school community, each isolated by the absence of shared language. Maria, the teacher, couldn’t find words that worked across professional boundaries and parental anxieties. David, the head of school, saw his investments in training and support undermined by linguistic chaos. A student struggled with “experiences” he couldn’t name, trapped between stigma and silence. A parent navigated Google searches and trial and error, desperate for frameworks that didn’t exist.
These aren’t isolated failures. They’re symptoms of a systemic infrastructure gap. The good news? The infrastructure exists. Schools can build mental health literacy that works across stakeholder groups. The challenge is understanding what that actually means and where to start.
Mental Health Literacy as System Infrastructure
Mental health literacy is often treated as individual knowledge: send teachers to a workshop, share resources with parents, deliver a lesson to students. But this approach misses the point. Individual knowledge becomes system infrastructure only when it converges on shared frameworks that allow different stakeholders to communicate effectively.
Think of it this way: if your school teaches three different maths curricula across three different year groups with no alignment between them, you haven’t built mathematical literacy. You’ve created confusion. The same principle applies to mental health. Literacy requires coordination, not just information distribution.
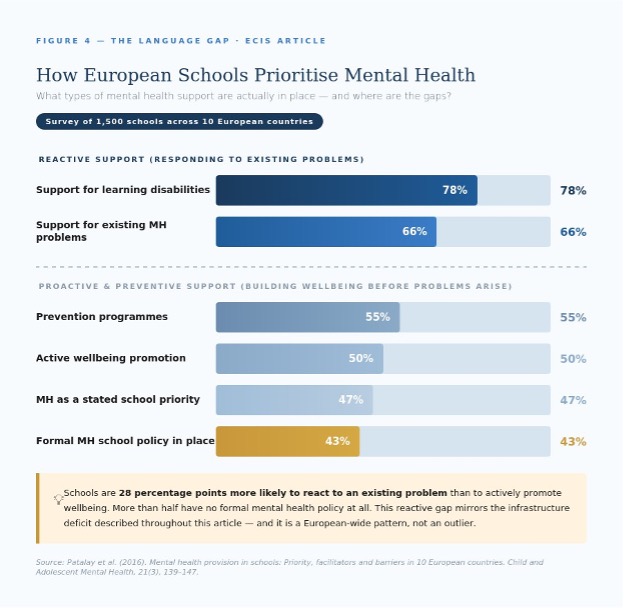
In a survey of 1,500 schools across 10 European countries, only 47% reported that mental health provision was a high priority, and more than half had no mental health school policy in place. (Patalay et al., 2016)
Support was overwhelmingly reactive: 78% of schools provided support for learning disabilities and 66% for existing mental health problems — but only 55% had prevention programmes and just 50% actively promoted wellbeing. (Patalay et al., 2016)
A 2025 European study found little consistency in how mental health is defined by decision-makers across schools, creating confusion and risk of inefficient or harmful implementation. (Nightline Europe, 2025)
Research consistently shows that educators feel ill-equipped to handle the growing responsibility of student mental health, citing insufficient training and lack of shared frameworks as primary barriers. (Springer, 2024; Skrzypek et al., 2024)
True mental health literacy means that everyone in your school community can: understand, access, and evaluate reliable information about mental health; recognise when behaviours or experiences warrant attention; differentiate between developmental, situational, and clinical challenges; reduce stigma through normalised, accurate language; make informed decisions about next steps; and promote psychological wellbeing proactively. Notice that none of these capabilities require clinical training. They require shared frameworks and agreed vocabulary.
The Three Spheres Framework
Effective mental health literacy operates across three interconnected spheres, each requiring its own foundation whilst aligning with the others.

Sphere One: The Home Environment
Parents need accessible frameworks for understanding adolescent development and mental health that don’t require clinical training but provide more structure than fragmented online searches. They need to differentiate between normal developmental challenges and signs that warrant professional support. They need vocabulary that allows them to communicate observations to schools without feeling they’re either overreacting or minimising genuine concerns.
When parents operate from the same foundational concepts the school uses, collaboration becomes possible. The parent from Part 1, searching “girl+14 years+no motivation+lazy+illness,” needs better starting points. She needs frameworks that help her observe patterns, communicate concerns effectively, and partner with school rather than operate in parallel.
Sphere Two: The Student Level
Young people need language that helps them understand their own experiences without pathologising normal emotions or, conversely, dismissing genuine distress. They need to know where reliable information lives. They need frameworks for distinguishing between temporary stress and persistent difficulties. And critically, they need this literacy delivered in ways that reduce stigma rather than reinforce it — normalising help-seeking rather than positioning it as an admission of weakness.
Half of all lifetime mental health conditions begin by age 15. Yet the majority of young people who need support never receive it — with stigma and limited mental health knowledge identified as the two dominant barriers.
(Radez et al., 2021; Gulliver et al., 2010; Rickwood et al., 2005)
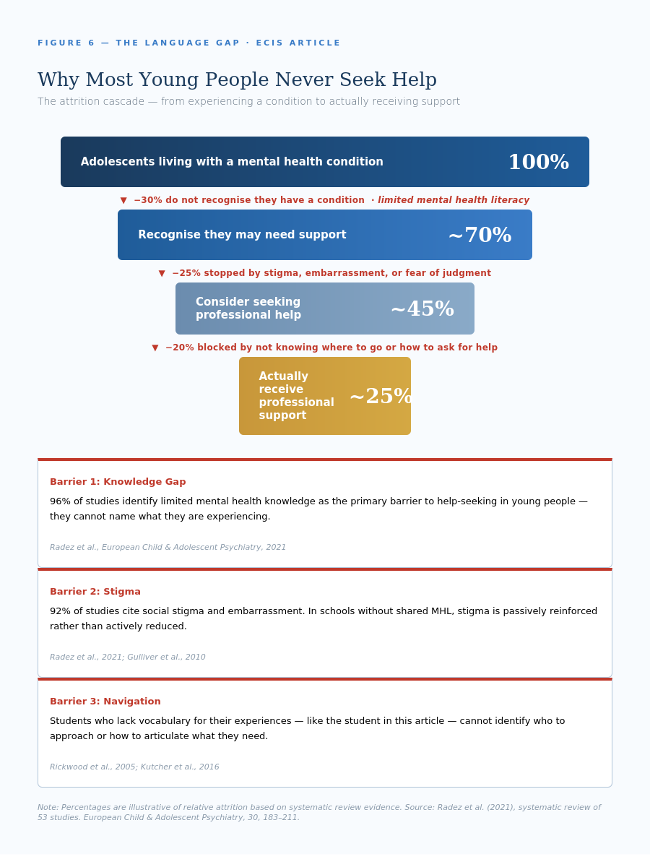
The student from Part 1 calls them “experiences” because he has no better vocabulary. He knows his “heart was pounding” and his “throat was dry” but doesn’t recognise these as anxiety symptoms with a name, a pattern, and available support. He’s trapped not just by his father’s “boys don’t cry” mentality but by his own lack of framework for what he’s experiencing. Student mental health literacy isn’t about self-diagnosis. It’s about self-awareness and navigation.
Sphere Three: School Staff and Leadership
Within schools, shared vocabulary needs to work across roles. Teachers need to describe observations without diagnosing. Pastoral coordinators need to triage concerns without creating bottlenecks. Counsellors need to guide interventions without operating in isolation. Leaders need to build systems that everyone can navigate confidently.
This requires more than training. It requires explicit agreements about foundational concepts and terminology that everyone uses consistently. When Maria’s colleague says “anxiety,” the counsellor says “emotional dysregulation,” and the deputy head says “resilience challenges,” they’re not describing different things. They’re using different dialects to describe the same student behaviours. The solution isn’t deciding who’s “right.” It’s establishing shared observational language that works across all three roles.
For leaders like David, this means auditing the linguistic landscape of your institution. What terms do different departments use for the same phenomena? Where do definitions diverge? What assumptions are you making about shared understanding that might not exist?
It Starts With You
Here’s the encouraging part: building mental health literacy doesn’t require waiting for whole-school transformation or district-wide initiatives. It starts with individual stakeholders taking responsibility for their own foundation.
If you’re an educator: Invest in your own understanding of adolescent mental health — not to become a clinician but to become literate in the landscape. Learn the frameworks your school’s counselling team uses so you can describe concerns in ways that connect to existing support systems. When you observe concerning behaviours, can you describe what you’re seeing in concrete, observable terms that avoid both clinical jargon and vague generalisations?
If you’re a school leader: Audit the linguistic landscape of your institution. Convene your counselling team, pastoral staff, and a cross-section of teachers. Ask them to describe the same hypothetical student scenario and compare the language they use. Where do terms diverge? Then build explicit agreements about observational vocabulary and ensure these are communicated to all staff, integrated into parent communications, and reflected in student-facing programming.
If you’re a parent: Seek out reliable sources and frameworks rather than assembling understanding from fragmented online searches. Engage with what your child’s school teaches about mental health and wellbeing. Build your own vocabulary so you can communicate concerns clearly and receive information without defensive reactions. Ask your school what frameworks they use and how you can learn them.
If you’re a student: Your role in building shared language is crucial. You can identify where adult frameworks fail to match teenage reality. You can name the stigma that keeps your peers silent. You can advocate for mental health literacy initiatives that actually resonate rather than feel performative. You can also take responsibility for your own literacy: learn to recognise your own patterns, understand when you’re struggling versus experiencing normal stress, and know where to access reliable information.
A Different Conversation
Let’s return to our four voices from Part 1, but now imagine them equipped with shared mental health literacy.
Maria — with shared literacy: Maria can describe Liam’s withdrawal using observational language that parents recognise as supportive rather than diagnostic. When she meets with Liam’s parents, she says: “I’ve noticed Liam seems less engaged over the past two weeks. He’s withdrawn from group work and seems preoccupied. These changes are worth paying attention to. What are you noticing at home?” The parents don’t become defensive because Maria’s language invites collaboration rather than implies diagnosis.
David — with shared literacy: David can implement support systems knowing that staff, parents, and students operate from aligned understanding. When he calls about the Grade 10 student, he doesn’t have to choose between competing framings. He uses the shared vocabulary the entire community understands: “Your daughter experienced acute distress in class today. Our nurse supported her through it and she’s doing better now, but this level of distress suggests we should talk about what support might help.”
The Student — with shared literacy: He now has language for his experience. He knows the difference between temporary stress and persistent anxiety. He can say: “I think I’m dealing with anxiety around performance and it’s affecting my ability to function.” He knows his school has a counsellor who specialises in exactly this. The stigma hasn’t disappeared entirely — but it no longer forms an impenetrable barrier because the entire school community talks about mental health using normalised, accurate language.
The Parent — with shared literacy: She can differentiate between typical teenage moodiness and signs of depression. She knows how to have conversations that invite openness. When she connects with school, she can say: “I’m noticing some changes that concern me — she’s more irritable than usual, sleeping more, and avoiding activities she used to enjoy. Can we talk about what you’re seeing at school?” The school recognises this language because it matches their own frameworks, and coordination follows naturally.
This is what shared mental health literacy makes possible. Not perfect systems or eliminated challenges, but coordinated support built on common understanding.
Starting Tomorrow
You don’t need to transform your entire school overnight. You need to take the first step toward shared language.
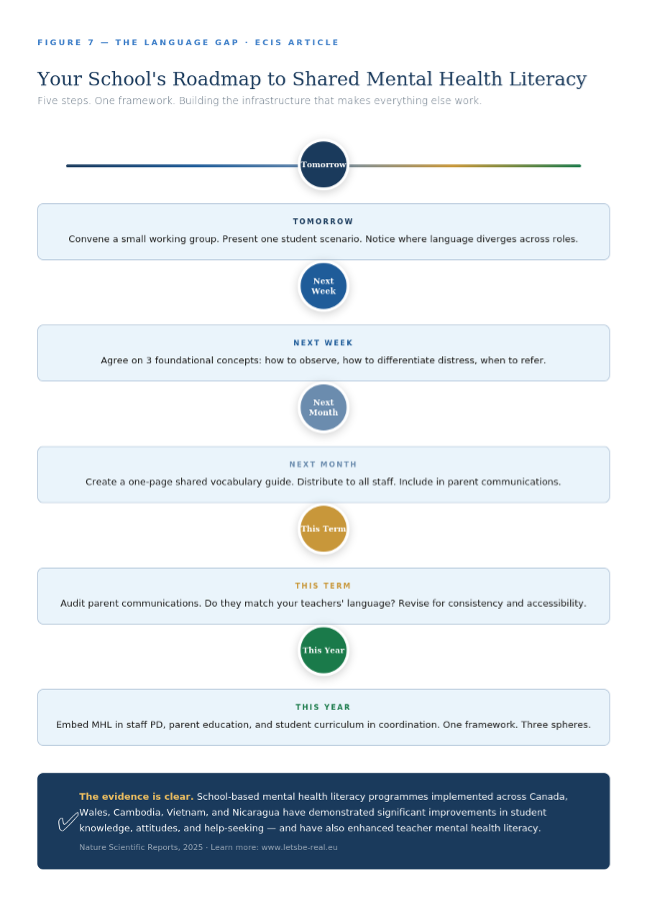
School-based mental health literacy programmes implemented across Canada, Cambodia, Wales, Vietnam and Nicaragua have demonstrated significant improvements in student knowledge, attitudes, and help-seeking — and have also enhanced teacher mental health literacy.
(Nature Scientific Reports, 2025 — international evidence review)
The infrastructure exists. The frameworks are available. The evidence base is strong. The question is whether your school will build the foundation that makes everything else work.
Because Maria shouldn’t have to translate between stakeholders. David shouldn’t be choosing between competing dialects. Students shouldn’t be trapped by vocabulary they don’t have. Parents shouldn’t be assembling understanding from Google searches.
They should all be having the same conversation, using the same language, working from the same foundation.
That’s what mental health literacy makes possible. And it starts with you.
The work of building shared mental health literacy in schools is challenging, but it is also essential. If your school community is ready to begin this work, we support educators, leaders, and parents in developing the frameworks and language that make coordinated wellbeing support possible. Learn more at www.letsbe-real.eu.
ABOUT THE AUTHORS
 Jacqueline Klemke
Jacqueline Klemke
Jacqueline M. Klemke is a Mental Health & Wellbeing Consultant, Mental Health First Aid Trainer, Systemic Coach, and co-founder of Let’s Be Real. Driven by a lifelong and deep passion for children’s mental health, she has dedicated her career to empowering young people, families, and educators with the emotional tools they need to truly thrive.
Her path to co-founding Let’s Be Real began as a parent, one who recognised the urgent need for better mental health and social wellbeing support within schools. That conviction led her to pursue specialised training as a Systemic Couples and Family Coach and Life & Business Coach, equipping her to work at the intersection of personal development, emotional literacy, and family dynamics.
🔗 Connect with Jacqueline on LinkedIn

Nick Praulins
Nick Praulins is a communication and learning consultant, certified Mental Health First Aid (MHFA) Instructor, and co-founder of Let’s Be Real. With over 20 years of experience in education and leadership, including time as a school leader, Nick brings deep expertise in helping individuals, teams, and organisations navigate change with clarity, confidence, and compassion.
His work spans classrooms and cross-cultural teams across Europe, where he specialises in turning complex strategies into communication and learning experiences that people genuinely understand and embrace. Recognising the urgent need for practical mental health support in schools, Nick co-founded Let’s Be Real to equip educators, parents, and young people with the shared language and tools to build psychologically safe, resilient communities.
🔗 Connect with Nick on LinkedIn
Let’s Be Real is a Frankfurt-based mental health education organisation dedicated to changing the conversation around mental health in schools. Founded by Jacqueline Klemke and Nick Praulins, Let’s Be Real delivers English-language wellbeing workshops and certified Mental Health First Aid (MHFA) training for international schools, families, and educators across Germany and Europe, both in-person and online.
At the heart of their mission is a simple but powerful belief: that young people deserve the tools to face the challenges of modern childhood, and that the adults in their lives deserve to be equipped to support them. Let’s Be Real addresses some of the most pressing issues facing today’s youth – social media pressure, identity struggles, stress, and disconnection – through evidence-based, practical, and deeply human programmes.
Their services include:
Certified MHFA training for school educators and parents
Wellbeing & resilience workshopsfor students, parents, and teachers
Parent education sessions focused on mental health awareness
Tailored school programsbuilt around each community’s unique needs
Proud members of ECIS (European Council of International Schools), Let’s Be Real is trusted by leading international schools across Europe as a go-to partner for building stronger, more connected school communities.
“Stronger, more connected communities through practical mental health education.”
🔗 Let’s Be Real on LinkedIn
www.letsbe-real.eu | Based in Frankfurt am Main, Germany
You might also like...
Storytelling as a way of mapping student learning
9th July 2024
Why Does Student Voice Matter in the Curriculum?
21st November 2023
Taking the long view: Sustainability for global citizenship transformation
28th May 2024
What is the value of personal knowledge? Reflecting on 17 years as an Army spouse
19th February 2024
AI & Back to School: The terms you agreed to over summer
12th May 2026