The Language Gap: Why Your School’s Mental Health Investments Aren’t Working
The Language Gap: Why Your School’s Mental Health Investments Aren’t Working
Jacqueline Klemke & Nick Praulins, co-founders, Let’s Be Real
The Scale of the Challenge: Global Evidence
- 1 in 7 adolescents aged 10–19 globally experiences a mental health condition — accounting for 15% of the global burden of disease in this age group. (WHO, 2025)
- Half of all lifetime mental health conditions begin by age 14. Three-quarters emerge before age 18 — making the school years the single most critical window for intervention. (WHO/UNICEF, 2024)
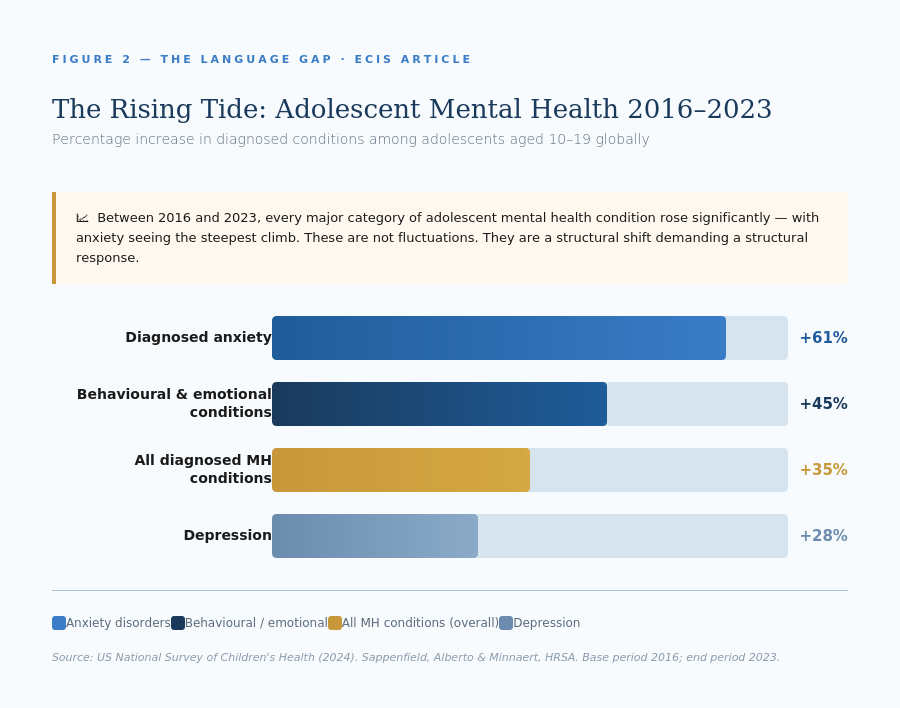
- Between 2016 and 2023, diagnosed mental or behavioural health conditions among adolescents rose 35% globally. Diagnosed anxiety increased by 61% over the same period. (US National Survey of Children’s Health, 2024)
- Yet more than 70% of people with a mental health condition receive no treatment at all — with lack of knowledge cited as a primary barrier. (Evans-Lacko & Thornicroft, 2013)

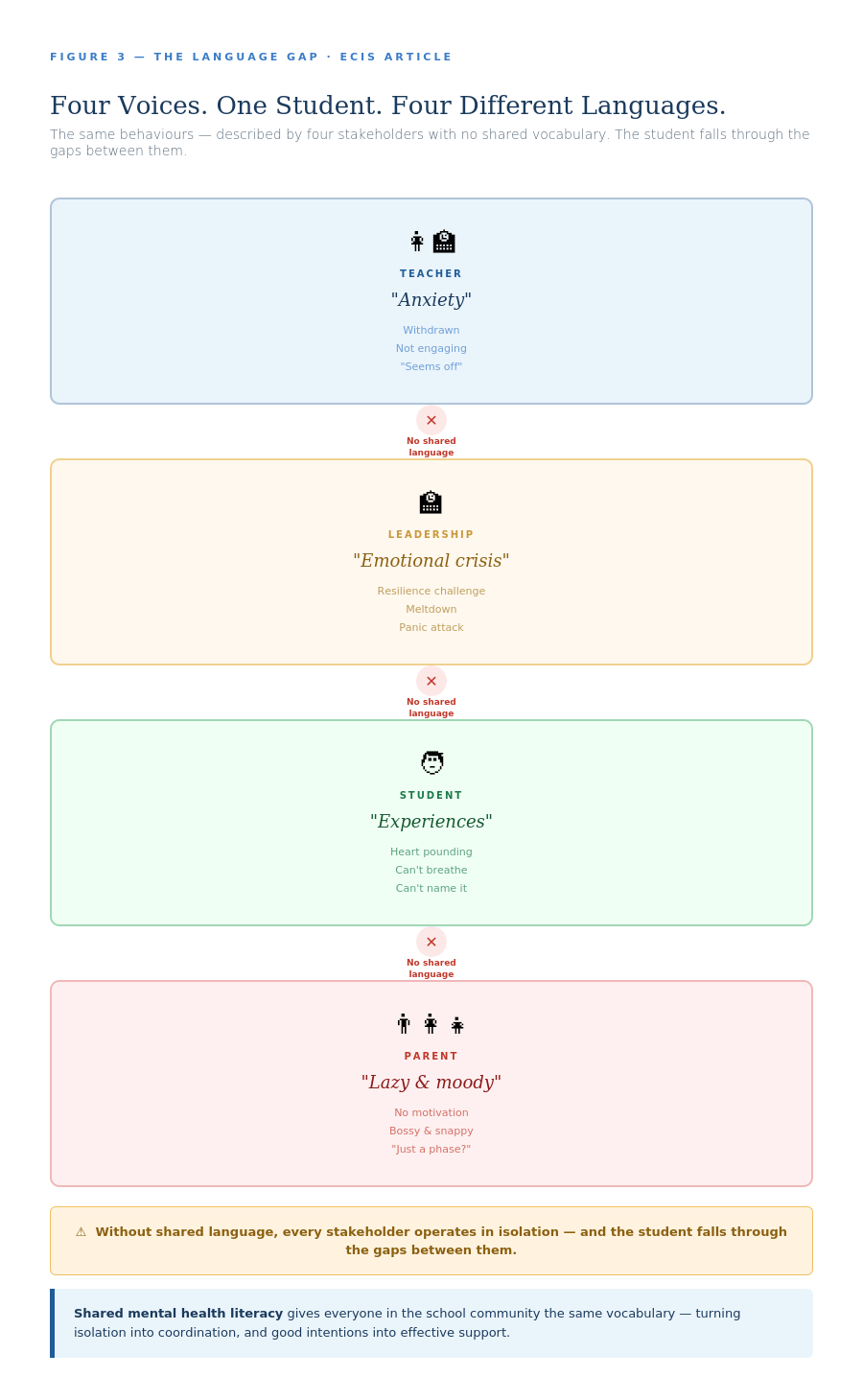
International schools invest heavily in student wellbeing. We hire counsellors, train staff, update policies, and convene wellbeing committees. Yet despite these efforts, many schools struggle to translate good intentions into effective support. The missing piece isn’t more resources or better programmes. It’s something more fundamental: a shared language that allows everyone in the school community to have the same conversation about mental health.Without this common vocabulary, each stakeholder operates in isolation. Teachers observe concerning behaviours but hesitate to name them. Leaders implement support systems that staff can’t confidently use. Students experience distress they can’t articulate.
Parents search for answers in a wilderness of conflicting information. The result is a system that works hard but doesn’t work together.This isn’t a failure of care or commitment. It’s an infrastructure problem. And like all infrastructure problems, it requires a systemic solution. That solution is mental health literacy, properly understood not as individual knowledge but as shared infrastructure.Mental health literacy, as originally defined by Jorm and colleagues (1997), refers to “knowledge and beliefs about mental disorders which aid their recognition, management or prevention.” This framework has since been expanded to encompass: understanding how to obtain and maintain positive mental health; recognising mental health difficulties and their treatments; reducing stigma; and enhancing help-seeking efficacy (Kutcher et al., 2016). Critically, mental health literacy is not about turning educators or parents into clinicians. It is about establishing common foundations that allow different stakeholders to communicate effectively about what they observe, experience, or feel concerned about.
But before we explore what that looks like in practice, let’s hear from four voices navigating the same school community without this shared framework.
The vignettes that follow are fictitious, but they are grounded in the real experiences we have encountered within the international school communities we have worked in and with. The patterns they reveal are not hypothetical. They are happening in schools across Europe and beyond right now.
From the Teacher Perspective: Maria’s Story
I noticed that Liam had become increasingly withdrawn over the past fortnight. When I mentioned it to his parents at a routine meeting, his mother immediately became defensive: “He’s just tired, not depressed or anything.” I tried to clarify (I wasn’t diagnosing anything, just observing a change) but the conversation spiraled. His father interjected that their GP said everything was fine, and they didn’t want the school “pathologising normal teenage behaviour.” I left the meeting frustrated, knowing something was off but unsure how to communicate my concern without triggering their protective instincts.Back in the staffroom, I vented to a colleague who suggested Liam might be “showing signs of anxiety.” But when I raised this with the school counsellor, she told me that without proper training, teachers shouldn’t use clinical terms. She preferred “emotional dysregulation,” whilst the deputy head later referred to the same behaviours as “resilience challenges.” Three different framings for the same student, and none of them creating a pathway for meaningful intervention.
This is what I wish you knew: I don’t need diagnostic precision. I need a common vocabulary that allows me, the parents, and the support team to have the same conversation. Without it, I’m translating rather than collaborating, and Liam gets lost in the gaps between our different languages.
From the Leadership Perspective: David’s Story
The incident report sat on my desk: a Grade 10 student had been escorted out of class after what the teacher described as a “complete meltdown.” The pastoral coordinator had documented it as an “emotional crisis.” The school nurse, who’d sat with the student afterwards, wrote “panic attack” in her notes. I knew I needed to call the parents, but which framing should I use? Each term carried different implications — and different levels of alarm.
I’d seen this pattern repeat itself throughout the term. Staff wellness surveys showed teachers felt underprepared to discuss mental health, yet they were increasingly expected to identify and respond to student struggles. Some erred on the side of caution and over-referenced; others, worried about overstepping, said nothing at all. Meanwhile, parents complained about mixed messages: one teacher would reassure them their child was fine, whilst another would suggest immediate intervention. We’d invested in training, brought in specialists, and updated policies, but without a shared framework that everyone could use confidently, each stakeholder was essentially speaking a different dialect.
This is what I wish you knew: No amount of goodwill will bridge this gap. We need a common language that works across roles, not just within them. Until everyone in our community can describe what they’re seeing using the same foundational concepts, we’re building support systems on unstable ground.
From the Student Perspective: A Student’s Story
I had another one of these strange “experiences” this morning. I was supposed to leave for school, but I could not. My heart was pounding. My hands were sweaty. My throat was dry. I could hardly breathe. The thought of going to school and failing, again, left me motionless. This was not the first time. I have been having these “experiences” ever since the two matches I lost as captain of the football team.
I think I might need help. But if my friends ever find out I am seeing a therapist, I will be done.
This is what I wish you knew: I think too many boys grow up believing in outdated role models. It takes a toll on them. It takes a toll on me. I wish I could allow myself to be vulnerable every once in a while. I wish I knew what to do, or who to talk to. Where to find information. I want to get better, but I don’t know how.
96% of studies on adolescent help-seeking identified limited mental health knowledge as the primary barrier. 92% cited stigma and embarrassment.Radez et al., European Child & Adolescent Psychiatry, 2021 — systematic review of 53 studies
From the Parent Perspective: A Parent’s Story
The other day I completely lost it. My 14-year-old daughter has been intentionally late for school on most days, spending all her afternoons on the sofa scrolling TikTok, not going out with her friends like she used to. She’s bossy and snappy. And I don’t know why.
Not knowing what else to do, I google “girl+14 years+no motivation+lazy+illness.” I am intimidated by the number of hits and what I read. “Lazy teen sloth.” “Diagnosing motivation problems.” “Motivating a teenager with depression.” Depression. My thoughts start racing.
This is what I wish you knew: Parenting a teen in 2026 is hard. I try to have all the answers, but I feel like it’s all still pretty much trial and error. I wish there was someone who could explain this teenage thing to me. I wish I understood teenage mental health better.
The Pattern Beneath the Stories
These four voices reveal something crucial: the absence of shared language doesn’t just create communication problems. It creates isolation at every level of the system.The teacher can’t advocate effectively for her student because she lacks vocabulary that bridges professional observation and parental understanding. The leader can’t build coherent support systems when every stakeholder describes the same phenomena differently. The student can’t seek help because he has no framework for understanding what he’s experiencing or where to turn. The parent can’t support her daughter because she’s navigating a wilderness of online noise without a compass.
The Real Cost of the Language Gap
Adolescents with a diagnosed mental health condition are 3× more likely to be disengaged from school, 5× more likely to miss 11 or more school days annually, and 10× more likely to have significant difficulty making or keeping friends. (US National Survey of Children’s Health, 2024)• Globally, 12 billion working days are lost every year due to depression and anxiety — at a cost of US$1 trillion in lost productivity. Today’s adolescents are tomorrow’s workforce. (WHO, cited in Nightline Europe, 2025)
Notice what’s not happening in these stories. No one lacks care. No one is refusing to help. Everyone is trying. But they’re building on different foundations, using different blueprints, speaking different languages. The result is a system that exhausts its participants whilst failing to deliver coordinated support to the young people who need it most.
This is what happens when mental health literacy is treated as individual knowledge rather than systemic infrastructure. We train counsellors. We send teachers to workshops. We share articles with parents. But if these efforts don’t converge on a shared framework, they simply add more voices to the cacophony.
Mental health literacy, properly understood, is not about turning everyone into amateur psychologists. It’s about establishing a common foundation that allows different stakeholders to communicate effectively about what they’re observing, experiencing, or concerned about. It means understanding how to access and evaluate reliable information. It means being able to recognise when something warrants attention and differentiate between different types of challenges. It means reducing the stigma that keeps students silent and parents defensive. And critically, it means being equipped to make informed decisions about next steps and to promote psychological wellbeing proactively, not just reactively.
“The question is: what would it look like if everyone in your school community could have the same conversation about mental health?”
Coming in Part 2: We explore the three spheres framework for building mental health literacy across your school community, with practical steps for teachers, leaders, parents, and students. We’ll return to our four voices and imagine how their experiences transform when everyone operates from shared understanding. Because the infrastructure exists. The question is whether your school will build it.
REFERENCES
Evans-Lacko, S., & Thornicroft, G. (2013). Mental illness stigma, help seeking, and public health programs. American Journal of Public Health, 103(5), 777–780. https://doi.org/10.2105/AJPH.2012.301056
Jorm, A. F., Korten, A. E., Jacomb, P. A., Christensen, H., Rodgers, B., & Pollitt, P. (1997). “Mental health literacy”: A survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Medical Journal of Australia, 166(4), 182–186.
Kutcher, S., Wei, Y., & Coniglio, C. (2016). Mental health literacy: Past, present, and future. Canadian Journal of Psychiatry, 61(3), 154–158. https://doi.org/10.1177/0706743715616609
Nightline Europe. (2025, February). Learning the lessons: Student mental health in Europe. https://www.nightline.fr/en/news/2025-02-03/student-mental-health-europe-new-report-nightline-europe
Radez, J., Reardon, T., Creswell, C., Lawrence, P. J., Evdoka-Burton, G., & Waite, P. (2021). Why do children and adolescents (not) seek and access professional help for their mental health problems? A systematic review. European Child & Adolescent Psychiatry, 30, 183–211. https://doi.org/10.1007/s00787-019-01469-4
Sappenfield, O., Alberto, C., & Minnaert, J. (2024). Adolescent mental and behavioral health, 2023. National Survey of Children’s Health Data Briefs. HRSA. https://www.ncbi.nlm.nih.gov/books/NBK608531/
Twenge, J. M., & Campbell, W. K. (2018). Associations between screen time and lower psychological well-being among children and adolescents: Evidence from a population-based study. Preventive Medicine Reports, 12, 271–283.
Valkenburg, P. M., Meier, A., & Beyens, I. (2022). Social media use and its impact on adolescent mental health: An umbrella review of the evidence. Current Opinion in Psychology, 44, 58–68.
World Health Organization. (2025). Adolescent mental health: Fact sheet. https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health
World Health Organization & UNICEF. (2024). Transforming the mental health of children and adolescents: A global framework for action. https://news.un.org/en/story/2024/10/1155536
ABOUT THE AUTHORS
 Jacqueline Klemke
Jacqueline Klemke
Jacqueline M. Klemke is a Mental Health & Wellbeing Consultant, Mental Health First Aid Trainer, Systemic Coach, and co-founder of Let’s Be Real. Driven by a lifelong and deep passion for children’s mental health, she has dedicated her career to empowering young people, families, and educators with the emotional tools they need to truly thrive.
Her path to co-founding Let’s Be Real began as a parent, one who recognised the urgent need for better mental health and social wellbeing support within schools. That conviction led her to pursue specialised training as a Systemic Couples and Family Coach and Life & Business Coach, equipping her to work at the intersection of personal development, emotional literacy, and family dynamics.
🔗 Connect with Jacqueline on LinkedIn

Nick Praulins
Nick Praulins is a communication and learning consultant, certified Mental Health First Aid (MHFA) Instructor, and co-founder of Let’s Be Real. With over 20 years of experience in education and leadership, including time as a school leader, Nick brings deep expertise in helping individuals, teams, and organisations navigate change with clarity, confidence, and compassion.
His work spans classrooms and cross-cultural teams across Europe, where he specialises in turning complex strategies into communication and learning experiences that people genuinely understand and embrace. Recognising the urgent need for practical mental health support in schools, Nick co-founded Let’s Be Real to equip educators, parents, and young people with the shared language and tools to build psychologically safe, resilient communities.
🔗 Connect with Nick on LinkedIn
Let’s Be Real is a Frankfurt-based mental health education organisation dedicated to changing the conversation around mental health in schools. Founded by Jacqueline Klemke and Nick Praulins, Let’s Be Real delivers English-language wellbeing workshops and certified Mental Health First Aid (MHFA) training for international schools, families, and educators across Germany and Europe, both in-person and online.
At the heart of their mission is a simple but powerful belief: that young people deserve the tools to face the challenges of modern childhood, and that the adults in their lives deserve to be equipped to support them. Let’s Be Real addresses some of the most pressing issues facing today’s youth – social media pressure, identity struggles, stress, and disconnection – through evidence-based, practical, and deeply human programmes.
Their services include:
Certified MHFA training for school educators and parents
Wellbeing & resilience workshopsfor students, parents, and teachers
Parent education sessions focused on mental health awareness
Tailored school programsbuilt around each community’s unique needs
Proud members of ECIS (European Council of International Schools), Let’s Be Real is trusted by leading international schools across Europe as a go-to partner for building stronger, more connected school communities.
“Stronger, more connected communities through practical mental health education.”
🔗 Let’s Be Real on LinkedIn
www.letsbe-real.eu | Based in Frankfurt am Main, Germany
You might also like...
More Connected Than Ever
4th June 2026
Taking the long view: Sustainability for global citizenship transformation
28th May 2024
Nurturing Student Agency in Secondary Mathematics: Challenges and Opportunities
17th June 2024
Rethinking Recess: 7 Steps to Foster Engagement and Inclusion
16th January 2025
Measuring Reading Fluency – Key Learnings from New Research
18th March 2025